Calcific Tendonitis
Calcific tendinitis is a relatively common cause of shoulder pain. It is characterized by the formation of hydroxyapatite deposits (a crystalline calcium phosphate) in any tendon throughout the body. They are most frequently encountered in the rotator cuff tendons of the shoulder. The exact cause/pathophysiology remains unclear with several mechanisms suggested. By one theory, it is postulated that the calcium deposits form as a pathologic response to tendon injury. Regardless of the cause, this clearly can be a very disabling and painful condition.

X-ray with calcium deposit above humeral head
The calcium deposits will vary in size from several millimeters (the size of a pea) to several centimeters in length and width. The size, chronicity, and position of the calcium deposit within the rotator cuff tendons will determine the magnitude and frequency of symptoms.
Calcific tendonitis progresses through stages from; formation, to latent (quiet stage), to resolution. On average, I would say that progression through these stages occurs in 1-3 years. Yes, a key point, the calcific deposit will spontaneously undergo natural resolution. There is no risk of migration, metastasis, and it is not contagious. Therefore, in the vast majority of cases I recommend conservative, (that is non-surgical) treatments.
The diagnosis will be suspected based on each patient’s history and physical exam, and confirmed with several simple X-rays that are done in the office on the day of your initial visit. Rarely is an MRI necessary to establish the diagnosis. Occasionally I will ask for an MRI if I suspect additional pathology or to confirm the exact extent and location of the calcium deposit within the rotator cuff tendon for treatment planning.

Ultrasound Image
In the acute stage, when the calcium deposit forms in the rotator cuff tendon, patients will experience intense pain around the shoulder. The rotator cuff tendon will become swollen and inflamed. There will be pain at rest and with general active shoulder motion. There is a propensity for catching and locking symptoms to develop as the swollen tendon rubs against or abuts against the under surface of the shoulder blade. This phenomenon is termed impingement syndrome, and in this scenario, the impingement relates to the rotator cuff tendon being too swollen or enlarged to freely travel beneath the acromial arch. Patients will often complain of being unable to move their shoulder through the normal range of motion related to sharp pain and catching sensations.
In the latent stage, there is much less swelling and inflammation of the rotator cuff tendon. Pain is generally less intense, and is noted mainly after vigorous use of the shoulder. (The pain developed after I racked my lawn or painted my house last weekend). Patients will notice discomfort primarily when they use the particular muscle/tendon that contains the calcium deposit. In the case of very large deposits, patients will experience catching and restriction of motion even during this relatively latent stage. Pain at rest is much less common during this stage. We will use simple in office X-rays to follow the deposit over time to help determine treatment plans.
Finally, the calcium deposit will begin the natural process of resolution. This stage is again marked by more acute inflammation and pain. The symptoms are similar to the acute developmental stage and the two stages can be very difficult to differentiate clinically. It is common for patients to present to the office during this stage.
Calcific tendonitis of the shoulder is relatively straightforward to treat. Surgery is rarely necessary and occasionally elected. The formation and resolution stages are notable for intense inflammation and pain, and as such, I usually recommend oral anti-inflammatory medication (such as Aleve/Advil). Frequently I will administer an ultrasound-guided steroid injection (similar to cortisone) to the region of the inflamed rotator cuff tendon and bursa. This can be extremely effective when acute pain and inflammation are present. During the quiescent, non-inflamed stage, I tend to recommend observation, and activity modification. By this, I suggest that patients perform light stretches twice per day to maintain shoulder motion. It is generally ok to use the arm/shoulder as needed for daily activities, but I recommend avoiding aggressive and highly repetitive lifting, pushing and pulling and in particular, repetitive above shoulder height use.
In refractory or extreme cases, there are two good options to remove the calcium deposit from the rotator cuff tendon. First, the ultrasound can be used to guide trephination of the calcium deposit. Under local anesthesia in the office, a needle is used to puncture the calcium deposit with several penetrations. This procedure stimulates leakage of the calcium out of the tendon and eventual resolution of the deposit in many cases. I usually combine this treatment with a steroid injection to help control pain. I advise light use of the arm for 2 weeks following this procedure to protect the healing tendon.
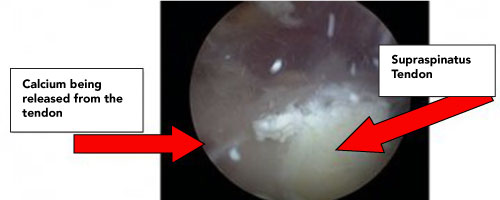
As a last option, when the situation dictates, the calcium deposit can be surgically removed. This is done by arthroscopic minimally invasive surgery. A small incision is created on the tendon in order to remove the calcium deposit and clean the rotator cuff tendon. Subsequently the defect in the rotator cuff tendon is repaired with suture to allow complete healing of the tendon in the region where the calcific deposit formerly existed. This procedure is highly effective but carries the standard risks of surgery and requires 4-6 months to fully heal the tendon.